
08/06/2025
Testosterone has anabolic effects on muscle (Figure 2A)3,4 and bone (Figure 2B)21 and stimulates erythropoiesis
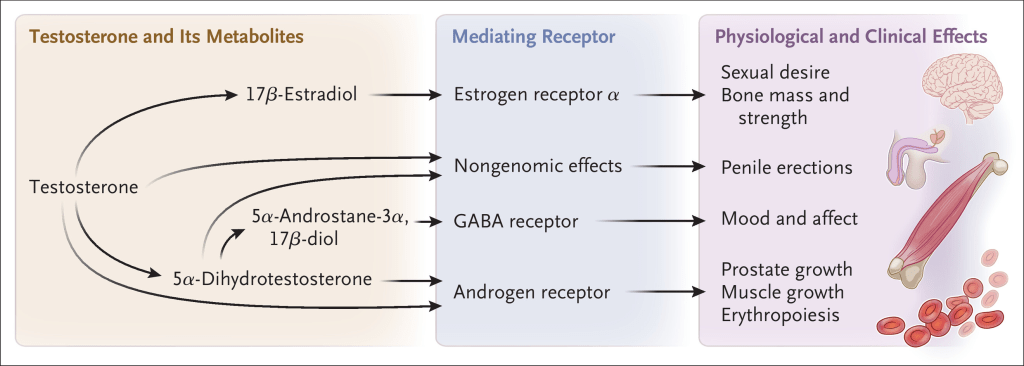
The effects of testosterone on sexual desire mediated largely through its conversion to 17β-estradiol.
Main null-outcomes reviewed:
Testosterone treatment did NOT increase the risk of major cardiovascular events among men with preexisting cardiovascular disease.
Testosterone treatment did NOT increase the risk of prostate cancer or acute urinary retention and did not worsen lower urinary tract symptoms.
History:
In 2003, a committee of the Institute of Medicine concluded that there was insufficient evidence that testosterone treatment in older men with hypogonadism had any clinically important benefit and recommended a coordinated set of trials to determine the efficacy of testosterone treatment in older men with hypogonadism
2 MAIN TRIALS OF HISTORICAL IMPORTANCE – TTrials + TRAVERSE
- TTrials
In response to this recommendation, a set of seven trials, the Testosterone Trials (TTrials), was developed to determine whether testosterone treatment in older men with hypogonadism would correct sxs.
790 men
~72 years old
baseline testosterone level was 234 ng per
Outcomes:
- increased sexual activity by approximately 40%
- libido by approximately 25%, and erectile function by approximately 35%
- modest improvements in physical function when evaluated with participant-reported or performance-based measures of walking – did not occur in men who walked slowly before treatment..
- did not improve the balance between vitality and fatigue
- hemoglobin level increased by at least 1.0 g per deciliter
2. TRAVERSE
Testosterone Replacement Therapy for Assessment of Long-Term Vascular Events and Efficacy Response in Hypogonadal Men (TRAVERSE)
5204 men
63 years
227 ng per deciliter
- increased sexual activity and libido but did not improve erectile function.
- improved mood by 3 to 4% (10% at baseline)
- neither decreased the rate of progression to diabetes among men with prediabetes nor affected glycemic control in those with overt diabetes
————————————-
MACE:
studies and some meta-analyses46,68 were limited by heterogeneity in the study populations, treatment regimens and duration, and testosterone levels during treatment, as well as by failure to adjudicate cardiovascular events.
TRAVERSE specifically targeted these outcomes:
- primary – MACE composite
- P<0.001 for noninferiority – numerically lower in treatement
- meta-analyses of testosterone trials have not shown a consistent relationship between testosterone treatment and the risk of atrial fibrillation
————————————-
PROSTATE CANCER
TTRIAL: prostate cancer was diagnosed in 3 of 335 men in the testosterone group (0.9%) and in 1 of 318 men in the placebo group (0.3%)
TRAVERSE
12 of 2596 men in the testosterone group (0.46%) and in 11 of 2602 men in the placebo group (0.42%)
Testosterone treatment increases PSA levels and thereby increases the likelihood that a prostate biopsy will be performed, which in turn increases the risk of detecting low-grade prostate cancer.
both trials excluded men at high risk for PCA – (elevated PSA)
In the TRAVERSE trial, the rate of increase in PSA levels after 12 months of treatment was similar in the testosterone and placebo groups
The incidence of acute urinary retention and initiation of new pharmacologic therapies for benign prostatic hyperplasia did not differ significantly between the groups.
————————————-
Synopsis:
decision of whether to recommend testosterone treatment should be made with an approach that balances the benefits and risks of treatment

- The lower the testosterone level (e.g., <200 ng per deciliter, the greater the likelihood of a benefit.
- A benefit is less likely in men whose testosterone levels are only slightly below the lower limit of the normal range, especially men with obesity and metabolic disorders
- older men for whom testosterone treatment is being considered should undergo a baseline evaluation for the risk of prostate cancer and for lower urinary tract symptoms.
- trials have not shown that testosterone treatment increases the risk of prostate cancer or lower urinary tract symptoms, men at high risk for those conditions were excluded from the trials.
- prophylactic anticoagulant therapy should be considered before testosterone treatment is initiated in men with a previous thromboembolic event.
- The decision to prescribe testosterone for a middle-aged or older man with hypogonadism should be guided by the degree of hypogonadism, the type and severity of symptoms, and the patient’s willingness to accept the risks of treatment and monitoring.
